Benign Paroxysmal Positional Vertigo - BPPV
Contents:
What is BPPV?

Benign Paroxysmal Positional Vertigo or BPPV is the most common cause of vertigo
- Benign: not dangerous or likely to cause lasting effects.
- Paroxysmal: rapid onset, reaches a peak and then slowly goes away.
- Positional: triggered by changes in head position.
- Vertigo: abnormal sensation of movement - world or self.
The inner ear balance system:
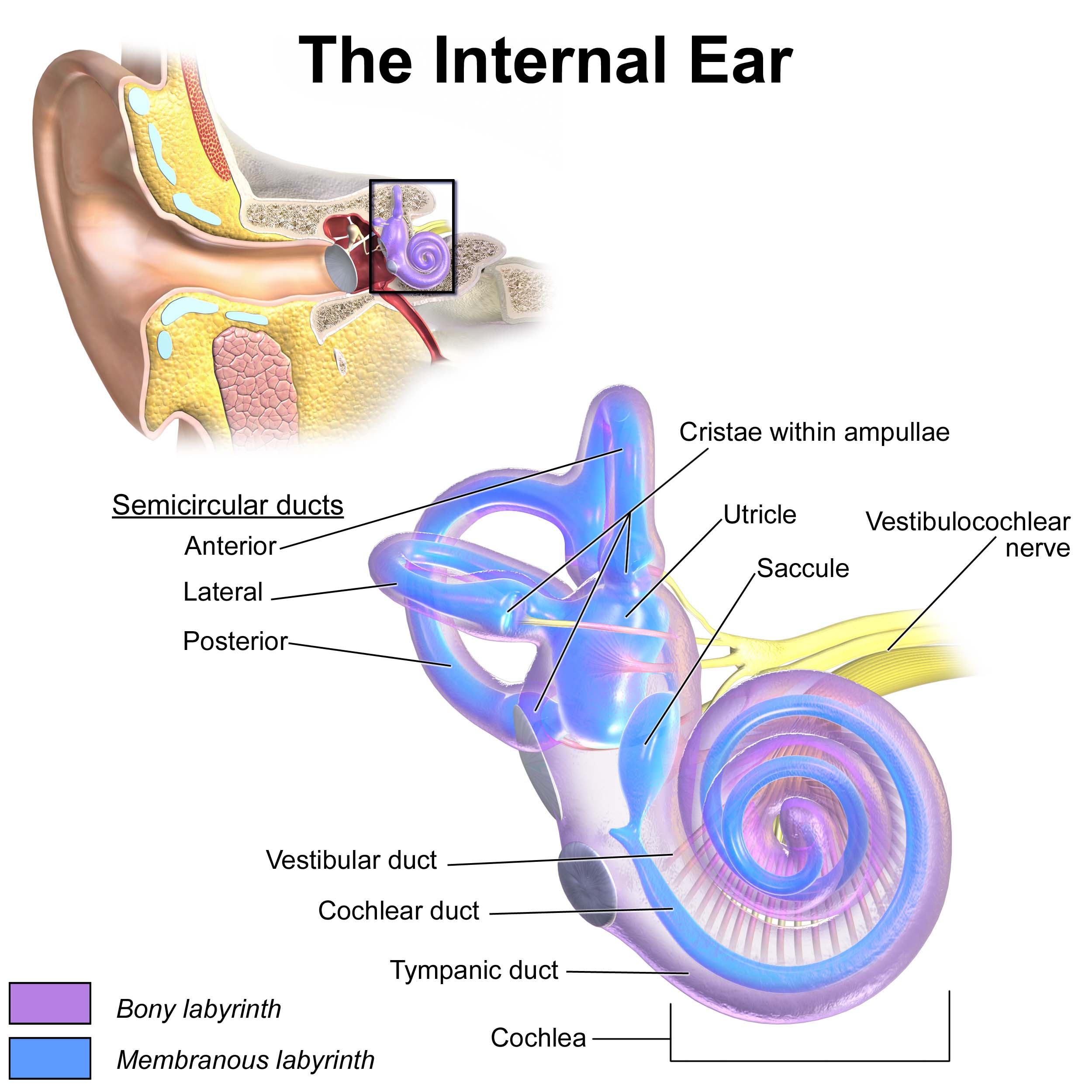
The entire inner ear system, cochlea (hearing) and vestibular (balance) apparatus, is encased in bone inside the skull and consists of delicate membranes filled with fluid.
The inner ear consists of 5 balance organs:
- 3 motion sensors called the semi-circular canals (horizontal, posterior and anterior canals).These canals are filled with fluid and contain motion sensitive hair cells.
- 2 structures which sense gravity and tilt called the utricle and saccule.
Moving the head makes the fluid flow through the semi-circular canals and stimulates the motion sensitive cells. This enables the brain to interpret direction and speed of head movement. The inner ears help control the eyes during head movement to maintain focus. When there is an inner ear dysfunction, it causes a reflex eye movement called nystagmus. The brain perceives this eye movement as a sense of motion so you experience dizziness i.e.: vertigo.
What happens in BPPV?
Small crystals of calcium carbonate are normally attached to the utricle & saccule in the inner ear and help the brain sense gravity. These crystals sometimes fall off into the fluid following a head trauma, viral infection or as part of the ageing process. Mostly the reason the crystals fall off in unknown. They drift into the semi-circular canals where they do not belong. The presence of these crystals within the semi-circular canals causes abnormal stimulation of the nerve endings when the head is moved and you experience vertigo.
Diagnosis
- The common diagnostic tests are the Dix-Hallpike test for the posterior canals and the roll test for the horizontal canals.
- These manoeuvres move the affected person into a position to cause vertigo and nystagmus (eye movement) by moving the crystals within the affected canal with gravity.
- The key to accurate diagnosis is determining which canal is affected. The direction of nystagmus indicates the affected canal, as in each canal the eyes beat in a specific direction. The correct treatment manoeuvre can then be performed for the affected canal.
Common Triggers of BPPV
- Getting in and out of bed
- Rolling over in bed
- Washing your hair in the shower
- Bending over in the garden
- Looking up or down into cupboards
- Hanging clothes on the line
- Looking down while reading or doing the washing-up
- Climbing up and down ladders
- Standing up or turning quickly
Characteristics of BPPV
- The vertigo is typically brief usually lasting no more than 10-60 seconds.
- The attacks usually occur in bouts which may last for 2-3 days or persist for weeks or several months at a time.
- Usually symptoms are worse in the mornings.
- Other symptoms may include nausea, vomiting, a sense of being off balance and light headedness.
- Hearing loss should not occur in BPPV. If you have noticed recent hearing loss in one ear, alert your GP as you should be sent for a hearing test to rule out more serious problems.
- Each semi-circular canal will cause a specific reflex eye movement when affected by BPPV. The direction of these eye movements tells the therapist which ear is affected and which canal the problem is in.
- BPPV can affect both ears at the same time but this is relatively rare and is usually seen after some type of head injury or fall.
Treatment of BPPV
- The treatment involves procedures called particle repositioning manoeuvres.
- These manoeuvres involve turning the head in different directions to use gravity to move the crystals out of the canal to be reabsorbed over time.
- Particle repositioning manoeuvres are the most effective treatments for BPPV
- In most cases, the manoeuvres are successful on the first attempt. In some persistent cases it can take two or more repositioning manoeuvres.
- Take care when performing the repositioning manoeuvres to have the head in the correct positions. In some cases if the manoeuvre is performed poorly the crystals may move out of one canal and into another. This can then take longer to clear.
Following treatment
- Keep your head still for approximately 30mins after the treatment to allow for the crystals to reabsorb (do not lie down, bend over etc). After 30mins you can resume your normal activities.
- In mild cases where the clinician has been unable to determine which canal is affected, you will be given some exercises to do each day until symptoms clear.
- Usually once the debris has been moved out of the canals, the residual symptoms of light headedness, nausea and imbalance will disappear in a couple of days.
- When BPPV has been successfully treated and you are clear of symptoms make sure you get on with life and forget about the BPPV, no matter how debilitating it may have been.
- Physical activity such as walking can help in the recovery.
Will BPPV come back again?
- BPPV can occur as an isolated event but it does have a tendency to reoccur. If it does either see your GP or refer yourself to the physiotherapist who treated you.
- Nothing can be done to stop recurrent bouts of BPPV so do not limit your activities just in case it does come back!
Conclusion
- In rare cases BPPV is resistant to treatment. Exercises can help minimise symptoms.
- Surgery is RARELY required or recommended.
- Drugs can be useful for the nausea, but will do little for the vertigo.The drugs STEMETIL, BUCCASTEM, PROCHLORPERAZINE and ANTINAUS should only be taken for brief periods. Check with your GP if you are taking any of these medications.